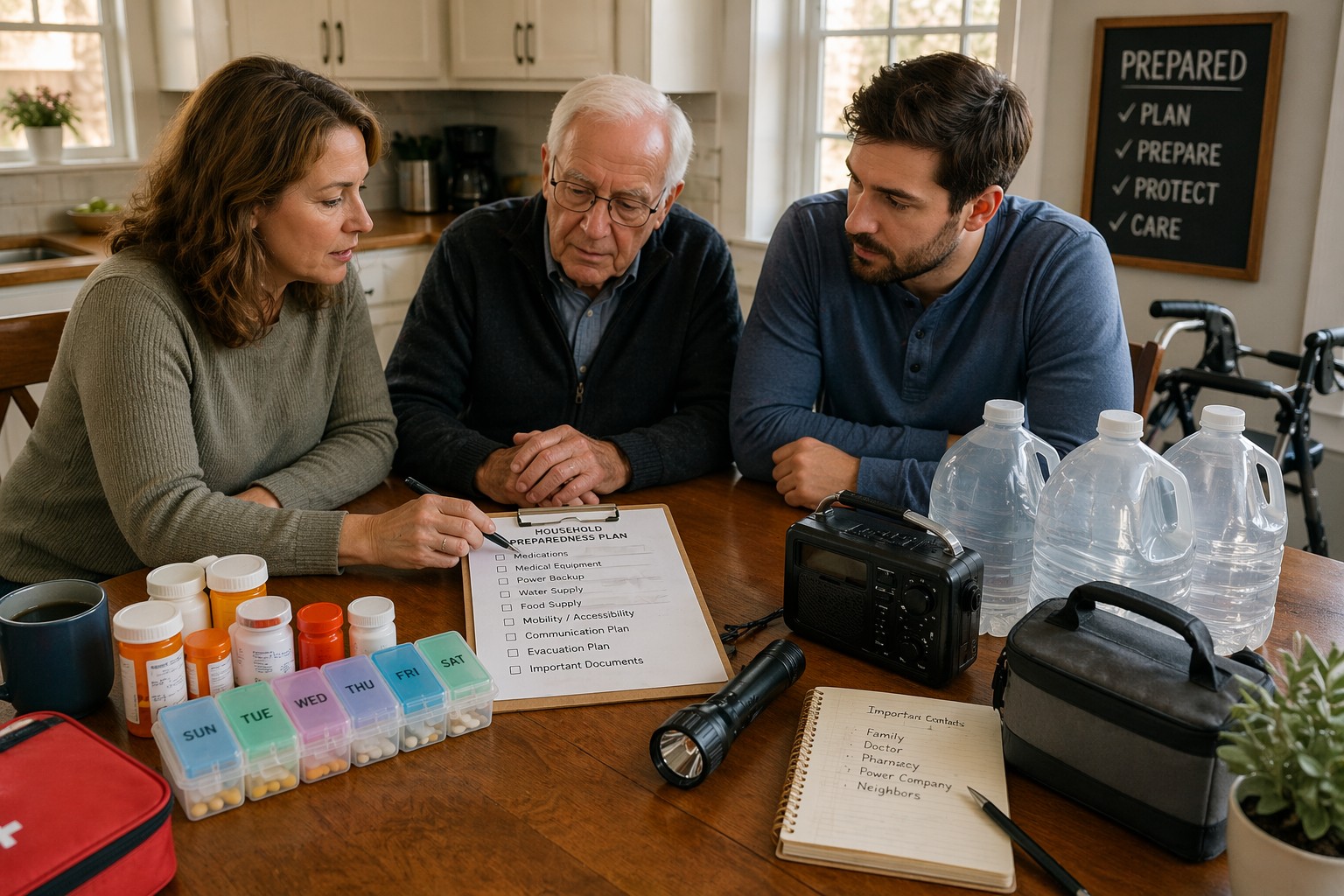
Household Preparedness for Elderly Parents and Dependents
Preparedness changes completely when elderly parents, children, disabled family members, or medically dependent household members are part of the plan. Power outages, water disruptions, transportation problems, and delayed emergency response create much greater risk when medications, mobility, medical equipment, or caregiving routines cannot fail safely.
Strong household preparedness means planning for the people who cannot simply “adapt later.” The goal is not just protecting supplies—it is protecting continuity for the people whose daily stability depends on systems working correctly before disruption begins.
Many households prepare for emergencies as if every person can respond the same way. That assumption fails quickly when medication schedules, oxygen equipment, refrigerated prescriptions, mobility limitations, memory challenges, or transportation dependence are part of daily life. Small disruptions become major emergencies much faster.
Preparedness starts by identifying what cannot fail safely. Backup power, water continuity, communication routines, transportation plans, and early evacuation decisions become far more important when dependents rely on stability instead of flexibility.
Identify What Cannot Fail Safely
Preparedness planning changes when someone in the household depends on medications, refrigerated prescriptions, oxygen equipment, mobility support, memory routines, or caregiver assistance. These are not “nice to have” systems—they are non-negotiable continuity points that cannot fail safely.
The first step is identifying what creates immediate risk if normal services stop. If power loss affects oxygen support, medication refrigeration, mobility lifts, or critical medical devices, backup planning must begin there—not with general supplies or convenience purchases.
Power, Water, and Medication Come First
For elderly parents and dependents, the first priority is usually not general preparedness—it is protecting the systems that keep daily life medically and physically stable. Backup power, drinking water, medication continuity, refrigeration, sanitation, and communication all become immediate priorities because delay creates higher risk much faster.
A common mistake is focusing on broad emergency supplies before protecting the systems that support health and caregiving. Strong preparedness starts by making sure the household can safely maintain medication schedules, hydration, temperature control, and essential equipment if disruption begins today.
Backup Power for Critical Medical Needs
If medications require refrigeration, oxygen systems need power, mobility devices require charging, or medical equipment cannot fail safely, backup power becomes a medical priority—not a convenience purchase. The goal is protecting life-supporting function, not restoring normal comfort.
The real question is not whether backup power exists, but whether it can protect critical medical needs for the full outage window. If refrigeration fails overnight, oxygen support becomes uncertain, or mobility equipment cannot recharge, the weak point has already been identified and must be solved immediately.
Prepared households know exactly which devices must stay powered, how long backup systems can realistically support them, and what happens if outages extend beyond that window. A common mistake is owning backup equipment without knowing whether it actually protects the dependent person’s daily stability.
Water Continuity for Health and Caregiving
Water planning becomes far more serious when medication routines, hygiene support, sanitation assistance, or mobility limitations are involved. Drinking water is only part of the problem. Bathing, toileting, cleaning, and safe caregiving routines all depend on reliable access.
The real test is identifying when normal care routines begin to break down. If stored water supports drinking but sanitation fails after one or two days, or hygiene needs become unsafe before refill options return, the weak point is not storage volume—it is continuity planning.
Prepared households calculate how long real care routines can continue if refill access stops. A common mistake is counting stored water without understanding how quickly dependent care creates higher daily demand.
Medication Access and Refill Protection
Medication disruption creates emergencies faster than most households expect. Prescriptions, refill timing, pharmacy access, refrigeration requirements, and transportation to appointments all become risk points during outages or evacuation pressure.
The real test is identifying what happens if normal refill access stops for several days. If a delayed prescription, missed appointment, refrigeration failure, or transportation problem creates immediate health risk, that weak point must be solved before disruption begins.
Prepared households protect medication continuity before disruption happens by tracking refill windows, written medication lists, backup provider contacts, and transportation plans. A common mistake is assuming normal pharmacy access will always be available when needed most.
.
Communication and Evacuation Must Be Simpler
Preparedness plans often fail because they assume every person can respond quickly, remember instructions, travel easily, and adapt under pressure. That assumption breaks immediately when elderly parents, children, disabled family members, or medically dependent household members require slower decisions and stronger support.
Communication plans and evacuation decisions must become simpler, earlier, and clearer. Waiting too long creates confusion, missed medications, unsafe travel, and dangerous last-minute decisions that are far harder to solve once the disruption is already underway.
Written Plans Beat Verbal Plans
Memory challenges, stress, medication schedules, and fast-moving disruption make verbal planning unreliable. Phone numbers, medication lists, provider contacts, meeting locations, transportation plans, and emergency instructions should exist in simple written form that every caregiver can access quickly.
The real test is what happens if the primary caregiver is unavailable tonight. If nobody else can find medications, contact the right provider, explain medical needs, or continue the daily care routine, the weak point is not supplies—it is missing continuity instructions.
Prepared households reduce confusion by removing guesswork. A common mistake is assuming everyone “already knows the plan” when real emergencies prove otherwise.
Leave Earlier, Not Later
Evacuation becomes more difficult when mobility support, oxygen equipment, wheelchairs, walkers, children, or medication timing are involved. The household usually needs more time, not less. Waiting for certainty often removes the safest travel window.
Prepared households decide departure triggers early and leave while roads, fuel, visibility, and destination support still exist. A common mistake is using normal evacuation timing for a household that requires much more planning.
Caregiver Failure Is a Real Weak Point
Preparedness often focuses on supplies while ignoring what happens if the primary caregiver becomes unavailable. Illness, injury, travel interruption, or communication failure can create immediate instability if nobody else can maintain medications, routines, transportation, or medical support.
The real test is whether the household can continue functioning if the primary caregiver cannot respond for several days. If medications are missed, appointments fail, transportation stops, or medical decisions cannot be made safely, the weak point is not the emergency—it is caregiver dependency.
Prepared households build backup caregivers, written instructions, and simple continuity plans before disruption happens. A common mistake is treating one reliable person as the entire preparedness plan.
Return to Household Preparedness Systems